
.bh__table, .bh__table_header, .bh__table_cell { border: 1px solid #C0C0C0; }
.bh__table_cell { padding: 5px; background-color: #FFFFFF; }
.bh__table_cell p { color: #2D2D2D; font-family: 'Arial',Helvetica,sans-serif !important; overflow-wrap: break-word; }
.bh__table_header { padding: 5px; background-color:#F1F1F1; }
.bh__table_header p { color: #2A2A2A; font-family:'Montserrat','DejaVu Sans',Verdana,sans-serif !important; overflow-wrap: break-word; }
It’s hard to develop a defensible mental health business.
Many solutions are commoditised. Network effects, scale economies and switching cost are rare.
One of the few ways you can develop defensibility is through scientific credibility. The businesses with credibility close deals faster and raise more capital. And as they do this, they gain the resources and reach that allow them to develop more evidence and more credibility. Their defensibility compounds.
This asset of credibility is built by generating evidence that holds up under scrutiny.
When you can make defensible assertions about what your product does, you will win over stakeholders and close deals. If you can then build a collection of defensible evidence, your scientific credibility is elevated to a strategic asset. You become known as a business that can be trusted to deliver on what you put forward. And that brings success, especially in a market that is increasingly scrutinising solutions.
But when your evidence isn’t defensible, stakeholders poke holes and conversations quickly grind to a halt. It’s a horrible feeling to be sitting in a conference room and watch a deal die as you’re asked to defend a position you knew was shaky. When you find yourself in this situation, it’s already too late.
In this Hemingway Guide, Jen Huberty PhD joins us to provide a framework for building scientific credibility as a mental health business. Jen has spent over twenty years in both academic research and commercial digital health. She was Head of Science at Calm and has advised several of the world’s leading digital health businesses.
Use this framework to strengthen your evidence, close more deals and develop scientific credibility as a strategic asset.
Key Takeaways
- Scientific credibility is a company's ability to defend its evidence with structured, stage-appropriate support that withstands stakeholder scrutiny.
- It primarily operates at an assertion level — your ability to defend specific assertions.
- Done repeatedly and with discipline, it can become a strategic asset
- Scientific credibility requires four interdependent foundations: Problem, Population, Solution, and Outcomes. Weakness in any area undermines the entire structure.
- You can use these four foundations to conduct a gap analysis before stakeholders expose weaknesses. Investors, enterprise buyers, and partners will find the holes eventually.
- You should prioritise the assertions you want to make defensible by understanding which are critical to your near-term business goals.
- Strong outcome data alone leaves critical questions unanswered: "Works for whom?" "Why does this problem matter?" "Is your solution what's creating these results?”
- Different stakeholders probe different foundations; balanced evidence matters more than deep evidence in just one area.
- Evidence expectations evolve with stage of your business. What's appropriate at pre-seed differs significantly from what's expected at Series A or enterprise scale. The goal is not to reach RCT-level rigor, it's to have the right evidence for the decisions your stakeholders are making right now.
- Founders who build complete evidence before competitors gain a structural advantage.
Building Scientific Credibility
Scientific credibility is a company's ability to defend its evidence with structured, stage-appropriate support that withstands stakeholder scrutiny. It is not defined by publications or methodological complexity; it is defined by whether your evidence holds up when the people making buying, funding, or partnership decisions push back on it.
It operates at two levels:
The assertion level. Everything a company puts forward about the problem it solves, the population it serves, how its solution works, and what outcomes it produces should be defensible across the four foundations.
The company level. Credibility at the company level is the cumulative result of scientific discipline applied consistently over time.
In this Guide we provide a framework for developing credibility in your assertions. You can use it to stress-test specific positions (before stakeholders do). Do this consistently and with discipline and the company-level asset will follow.
The Four Foundations of Scientific Credibility
Scientific credibility is built on four distinct foundations. They are defensible independently and when combined, reinforce one another.
- Problem: The problem you’re tackling is real, defined, and quantified for a specific group
- Population: The evidence reflects the actual people you're trying to support
- Solution: Your product specifically drives the change, not something else
- Outcomes: The improvement is measured, meaningful, durable, and aligned with what your buyer cares about
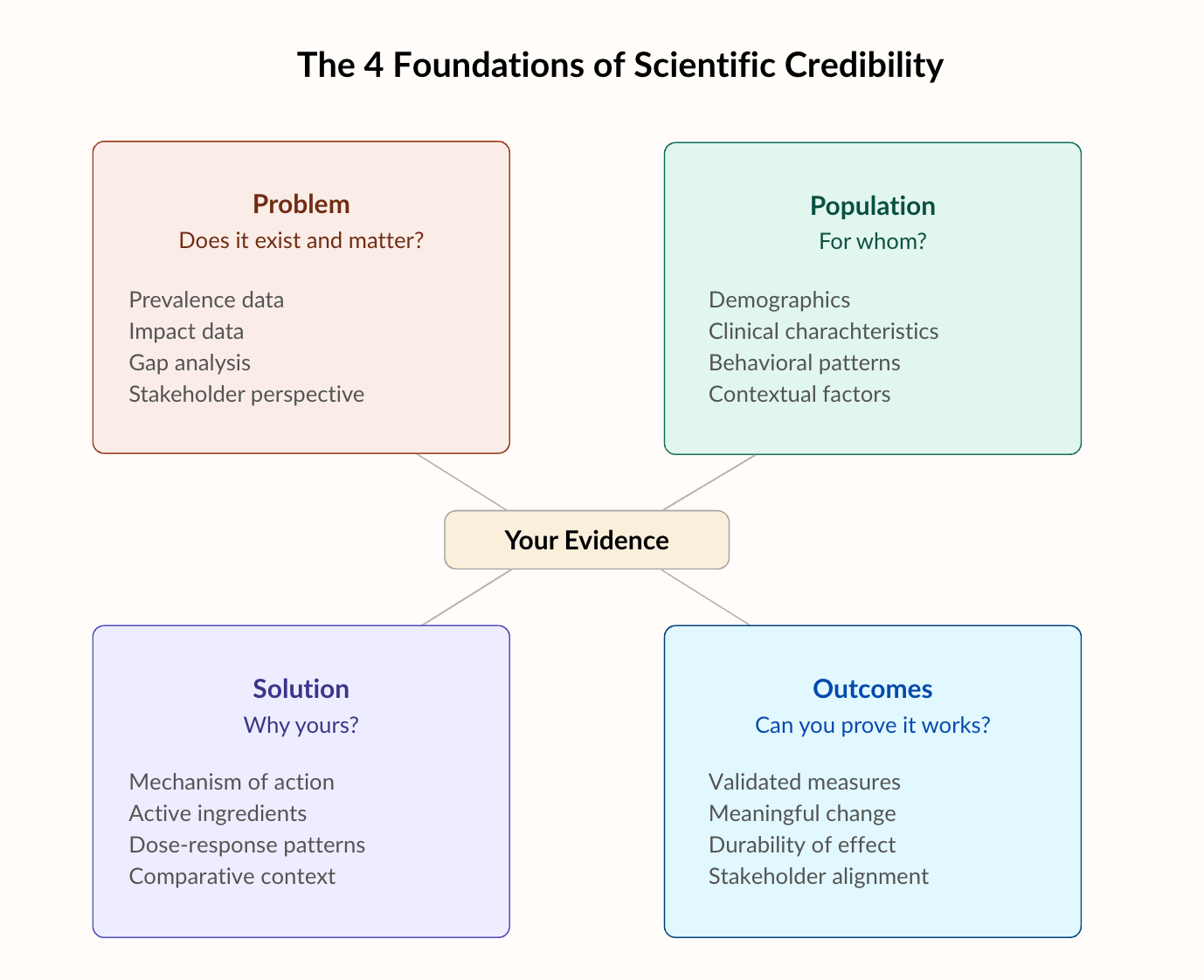
Figure 1: The Four Foundations of Scientific Credibility
When you have all four foundations for an assertion, you can say; this is a real, quantifiable problem with direct health and economic impacts for this specific population and our solution solves this problem through this precise mechanism, resulting in measurable improvements in the metrics you care about.
Example: "Untreated anxiety costs U.S. employers $4,400 per affected employee annually in lost productivity, disproportionately impacting hourly frontline workers with limited access to traditional therapy. Our platform delivers asynchronous CBT through a guided self-pacing model that produces a 40% reduction in PHQ-9 scores within eight weeks, sustained at six months".
Each foundation reinforces and strengthens the others, creating a more defensible and resilient evidence base. Together, they can support your business decisions and build your scientific credibility.
Building an evidence base can be expensive and takes time. Therefore, the best organisations know how to do two things well when it comes to scientific credibility;
- They understand which assertions they need to make to support their business goals.
- They know how to make those assertions highly defensible with strong evidence generation across all four foundations.
Prioritise the Assertions that Support your Business Goals
Figure 1 above showed how the four foundations apply to any single assertion. But most companies are defending multiple assertions simultaneously, each with different levels of evidence. Figure 2 (below) shows what that looks like in practice.
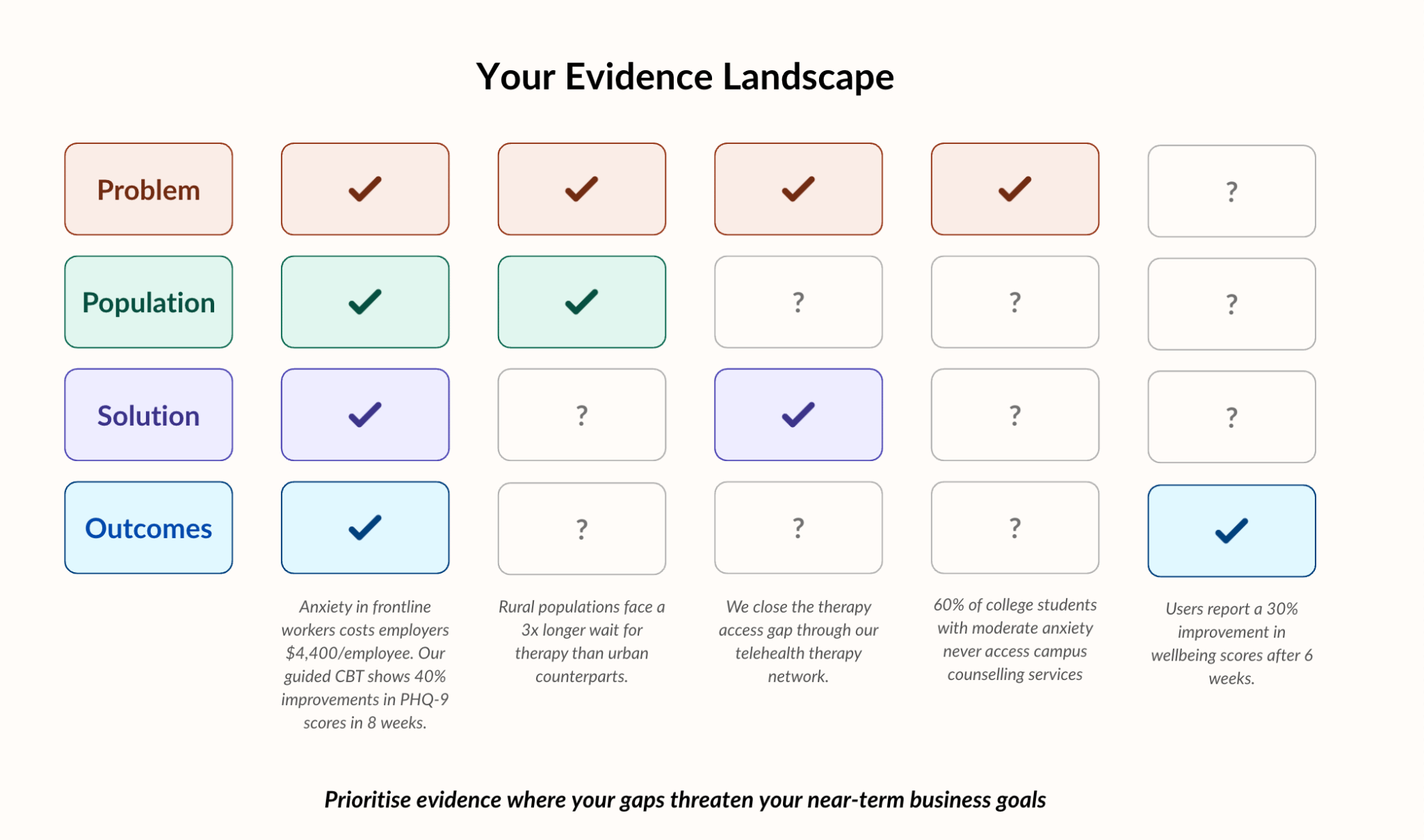
In reality, a company may have many more assertions than this, for different products and different stakeholders.
Thankfully, not all of these need to carry equal weight at any given moment. You need to understand which ones are critical to your near-term business goals and make sure those are structurally sound.
To do this, work backwards from your business strategy. Ask yourself, what business goals do I need to hit in the next twelve months and what will I need to defend to achieve them? Those are your priorities and should be the focus of your evidence generation strategy.
If your goal is to land five new enterprise contracts with employers, your assertion about reducing absenteeism is the one under pressure. If you only have problem and population evidence but no solution attribution or outcome data, that's your vulnerability. It doesn't matter that your investor-facing evidence is complete. The assertion that's being tested is the one that needs to hold.
Build in the Right Order
It’s unrealistic to build all four foundations simultaneously across every assertion or business decision. And you don’t need to. The ideal sequence depends on your stage and the conversations that are most critical right now.
Early stage (pre-seed / seed). You might have evidence across one or two foundations for a single assertion. That’s OK. No one expects a complete evidence base at this stage. Focus on having strong evidence for a specific problem and population. You need to prove the problem matters and understand who experiences it before you invest heavily in solution development.
Series A. You need at least one assertion that meets all four foundations, and credible foundations progress on other key assertions Solution evidence should be emerging from product development and feasibility testing. If you're planning a raise in twelve months, outcome data collection should start now.
Growth stage and enterprise scale. You need evidence across multiple assertions because you're selling to multiple stakeholder types simultaneously. The employer buyer, the health plan, the health system — they each care about different claims, and each of those claims needs to hold up independently.
When we worked with a national virtual mental health provider, they had strong problem validation, clear population definition, and a well-articulated solution, but needed rapid outcome evidence to support their growth stage. We analyzed 5+ million therapy visits and published four papers in three months showing clinically meaningful symptom reduction. That completed their evidence at exactly the right time for their business needs.
Using the Four Foundations to Build Defensible Assertions
Now that you know which foundations to prioritise and when, the rest of this guide is a detailed framework for assessing each one. Use it to assess the strength of your evidence within your most critical business conversations, and to identify where your evidence needs to be stronger.
Foundation 1: The Problem
Do you have evidence that the problem you are solving actually exists and actually matters?
Many founders start a business to solve a personal pain point. But personal experience or anecdotal evidence are not the same as defensible problem evidence. You need to be able to clearly define the problem, its prevalence, the impact of that problem in health and economic terms, and why existing solutions don't solve it.
What strong problem evidence looks like
Strong problem evidence rests on a small set of defensible components:
Prevalence data showing how many people experience the problem. Strong sources include peer-reviewed epidemiological studies, CDC and WHO surveillance data, large national surveys (e.g., BRFSS, NHANES), and some condition-specific registries. Avoid white papers or market research reports that cite prevalence without primary sources.
Impact data describing consequences in health, economic burden, or quality of life. Look to health economics literature, employer claims databases, and government cost reports (e.g., AHRQ, CMS). Self-reported impact data from your own users can supplement these sources but shouldn't be used as your primary source.
Gap analysis clarifying what current solutions exist and why they fall short. Strong support comes from systematic reviews and meta-analyses identifying intervention gaps, published critiques of current standards of care, clinical practice guidelines that acknowledge unmet needs, and competitive landscape analyses grounded in peer-reviewed efficacy data. High-level competitive summaries or marketing claims about differentiation are not sufficient on their own.
Stakeholder perspective confirming that users define the problem the way you do. Examples include structured needs assessments, qualitative research with target users and buyers, and published patient/member experience data. Anecdotal feedback from a handful of users is not stakeholder validation.
Prevalence and impact are only persuasive when they are clearly defined and specific. A problem may be widespread, but severity, contributing factors, and consequences often vary meaningfully across subgroups. If the problem is not clearly defined for a specific population, evidence becomes easy to challenge.
For example, a digital mental health company with strong UK adoption entered the U.S. market expecting their existing evidence to transfer. It didn't. Prevalence patterns, access barriers, and stakeholder expectations differed enough that general UK data wasn't sufficient to support adoption in this new market. They needed to develop U.S.-specific problem evidence, establish a U.S. advisory board, and publish research in the U.S. before the problem could be defended credibly with American buyers.
You must be able to clearly demonstrate that the problem is real, meaningful, and unresolved. Before including a new source in any material, the strongest teams pressure-test each one by asking: does this materially strengthen our ability to defend the urgency and specificity of this problem in a real business conversation?
When problem evidence is weak
There are several red flags that signal weakness in your problem foundation. One is when teams default to saying "everyone knows this is a problem" without quantifying the prevalence or impact within your defined population. It's also a red flag when a company describes the problem differently to how their target users do. And it's a mistake not to provide a concise articulation of why existing solutions fail.
Consider a stress management platform that cites national data on rising stress and burnout. That data is accurate. But when the company enters enterprise conversations with their target clients, the HR leaders they're selling to are focused on absenteeism, retention, and performance variability in specific teams. The company never clarified which subgroup experiences the most severe impact or how current solutions fail them specifically.
Without a defensible problem definition, messaging becomes generic and sales conversations stall under scrutiny. If stakeholders can't see why your solution should even exist in the first place, there's no point in talking about anything else.
Join the Hemingway Community
If you’ve read this far it’s probably because you want tactical information on building a successful mental health organisation? If you’d like more of that, and to meet peers building similar businesses, consider joining the Hemingway Community.
As a member of the community, you’ll join over 450 other mental health leaders and get access to exclusive content, events and resources.
Foundation 2: The Population
Does your evidence reflect the specific population you intend to serve and have you designed your product with them in mind?
Solutions that are effective for one population may fail for another. Stakeholders want to know whether your data extends across their broader employee, patient, or member population. If you cannot clearly define who your evidence applies to and who it does not, stakeholders will question its generalizability. Precision builds trust. Ambiguity weakens it.
What strong population evidence looks like
Strong population evidence typically includes clarity across four dimensions: demographics (age, gender, socioeconomic status, geography), clinical characteristics (severity, comorbidities, treatment history), behavioral patterns (health literacy, technology comfort, engagement barriers), and contextual factors (cultural considerations, access constraints, support systems).
It's about understanding the real-world conditions that shape whether your solution will be adopted and effective. This evidence is usually built through structured user research, disciplined customer discovery, segmentation analysis, literature on population-specific intervention effectiveness, and internal data confirming that your intended population is engaging as assumed.
The most credible population evidence moves beyond description into applicability. Demographic summaries or personal documents are not sufficient. Stakeholders want to see that your data reflects the population you are targeting and that engagement, usability, and early signals are consistent within that segment. The goal is distinguishing between who shows interest and who demonstrates sustained fit.
As an example, a pre-seed company ran a feasibility study with 19 patients and conducted focus groups with eight users to understand feature needs and retention drivers within that population. They also interviewed four healthcare providers to validate clinical fit. They came out of that knowing who their product may work for, what those users needed, and whether clinicians would endorse it for that group. The feasibility study became the foundation of their pitch deck and go-to-market messaging and played a key role in securing funding.
When population evidence is weak
The red flags are easy to spot. The product is described as broadly applicable — "our product is for everyone". There is no clearly defined core user. There are significant differences in engagement across demographic or clinical subgroups but they are unexplored. There is little data showing reach among the highest-need populations.
When population specificity is weak, the consequences tend to show up when you try to expand beyond your initial user base. The claims you used for your original users don't extend to the new group. This doesn't mean companies should avoid expanding into new populations. It means the evidence strategy needs to expand with them. Before entering a new segment, teams should understand the key differences between the population they have data on and the new population they're targeting, and have a plan for testing whether their core assumptions hold. Going into a new market with a credible evidence plan is a fundamentally different conversation than discovering misalignment after the deal is signed.
Foundation 3: The Solution
Does your specific solution solve the problem?
Improvement can occur for many reasons: natural symptom fluctuation, regression to the mean, concurrent treatments, or increased motivation simply from enrolling in a program. If you cannot demonstrate how your solution specifically drives change, your claims become vulnerable. In a crowded digital health market, attribution is often what separates credible differentiation from commoditized claims.
Another example… An AI mental health platform showed that over 60% of sessions produced measurable mood and stress improvements. On the surface, that’s promising. But mood naturally fluctuates, and users tend to initiate sessions when they're already feeling low, meaning some recovery would be expected regardless of the intervention. Without a comparison condition or a way to account for natural mood recovery, the question of attribution remained open. The results were difficult to defend in investor, partner, and buyer conversations. For this company, strengthening that link became the focus of their evidence strategy.
What strong solution evidence looks like
Before you claim impact, you need to articulate why your solution works. Strong solution evidence creates a defensible causal narrative, linking product design decisions to measurable change.
A clearly defined mechanism of action. This goes beyond naming a modality. It explains how specific features or interactions lead to measurable change. What is the behavioral, cognitive, or physiological pathway? How does engagement translate into outcomes?
Example: One youth mental health platform didn't just claim that therapy reduces symptoms. They articulated a specific multidisciplinary model combining individual therapy, psychiatric support, and family involvement and demonstrated how that integrated pathway led to symptom reduction in 80–95% of youth served. The mechanism wasn't "we offer mental health support." It was a defined clinical pathway with evidence for how each component contributed to change.
Clarity around active ingredients. Not every feature drives impact equally. Credible teams examine which elements are essential versus supportive and test whether modifying or removing components changes outcomes. This separates signal from noise.
Example: A mental fitness app offered cognitive games, guided exercises, personalized training, and progress tracking. Through structured evaluation, the team developed a scientific framework that identified which specific activities drove measurable cognitive improvement and which were supportive but not essential. That clarity allowed them to prioritize development resources, refine their product around what actually worked, and defend their differentiation with evidence rather than feature lists.
Dose-response patterns. If the solution functions as intended, greater engagement with core components should align with stronger outcomes. While dose-response does not prove causation alone, it strengthens the attribution argument.
Example: A virtual mental health platform analyzed data from millions of therapy visits and found that symptoms of anxiety and depression dropped meaningfully within five sessions, with continued improvement over time. Among patients with severe symptoms, the majority experienced clinically significant reductions within eight weeks. The pattern was clear: more sustained engagement with therapy sessions aligned with stronger outcomes, reinforcing that the platform's core service was driving change.
Comparative context. Improvement only means something relative to an alternative. Without a reference point, observed change is difficult to interpret. This may involve matched cohorts, historical baselines, comparisons to standard care, or industry benchmarks.
Example: A PTSD treatment platform analyzed outcomes from 148 adults receiving massed cognitive processing therapy — an intensive, compressed format — compared to the traditional weekly pacing of the same evidence-based treatment. Results showed significant improvement in PTSD symptoms, anxiety, and depression, with gains maintained at three months post-treatment. By comparing their delivery model against the established standard, the company could demonstrate that their approach offered a meaningfully different path to the same outcome.
When these elements align, you deliver a defensible explanation of how and why users improved. That explanatory clarity is what differentiates credible innovation from commoditized digital health tools.
When solution evidence is weak
When the solution is weak, differentiation becomes fragile. You may show improvement, but you cannot explain why your solution works or which components are responsible for outcomes.
A digital health company with 465 members had assessments that were not built on any scientific framework or foundation. There was no standardized member journey connecting solution components to expected outcomes. Without that, the company could not demonstrate which elements of their program were driving change. This made their evidence both difficult to explain and easy to challenge in stakeholder conversations.
The red flags are clear. Teams say "users improve when they engage," but cannot define what meaningful engagement actually is. Every feature is treated as equally important. Active ingredients are not identified. Improvement is assumed to be attributable to the solution without demonstrating causal linkage. Under scrutiny, the evidence looks correlational rather than product-specific. Without clear attribution, credibility and differentiation both weaken.
Foundation 4: The Outcomes
Can you demonstrate measurable, meaningful improvement in health, behavior or economic data?
This is often the first question stakeholders ask — does it work? Outcome data is important. But impressive numbers built on a vague problem definition, an undefined population, and no attribution mechanism will collapse under scrutiny.
A common mistake is focusing on collecting outcome data before creating the infrastructure needed to measure it properly. In these cases, teams collect a lot of data, but it's the kind of data that doesn't withstand deeper questioning.
What strong outcome evidence looks like
Strong outcome evidence rests on a disciplined measurement strategy. It is not just about showing change. It is about showing change that is interpretable, meaningful, durable, and aligned with stakeholder priorities.
Use of validated measures. Proprietary indices or internally created metrics may be useful operationally, but stakeholders expect standardized instruments when evaluating clinical or behavioral change. Learn more about validated measures in our other Hemingway Guide.
Appropriate measurement timing. Outcomes should be assessed when change would reasonably occur. Too short, and results lack interpretability. Too long without follow-up, and durability becomes unclear.
Clarity on meaningful change. A result can show measurable improvement without that improvement being large enough to matter in real life. Stakeholders want to understand whether the magnitude of change crosses clinically meaningful thresholds and translates into real-world impact.
Durability of effects. Short-term gains may reflect novelty or initial motivation. Sustainable credibility requires evidence that improvements persist beyond the initial intervention window.
Alignment with stakeholder priorities. If enterprise buyers care about absenteeism, productivity, or healthcare utilization, those outcomes must be visible in the evidence. If payers focus on risk reduction or cost offsets, measurement strategies should reflect those endpoints. Outcomes that are not stakeholder-aligned are easy to dismiss, even when statistically robust.
Proportional evidence progression. Early-stage companies may begin with self-reported improvements or engagement correlations. As the company grows, evidence should evolve toward structured pre-post change using validated instruments, then toward comparative effectiveness, durability of effects, and clinically meaningful thresholds. Understanding this progression helps teams calibrate expectations while strengthening credibility over time.
When outcome evidence is weak
When this foundation is weak, growth conversations slow. Engagement metrics may look strong. Satisfaction scores may be high. But measurable health improvement remains unclear.
A weight management platform reports modest short-term weight loss and high user satisfaction. When speaking with a self-insured employer, however, the buyer asks about sustained weight reduction, cardiometabolic markers, and impact on healthcare utilization. The company cannot demonstrate durability of effects beyond the initial program window. Outcomes rely on proprietary or non-validated instruments rather than standardized measures. There is little evidence that the reported changes align with the buyer's cost or utilization priorities.
The warning signs are not always about missing data — they are about weak interpretation and misalignment. Short-term gains are emphasized without follow-up data. Proximal indicators such as knowledge or awareness are measured instead of meaningful behavioral or clinical outcomes. Best-performing users are highlighted rather than average effects. Clinical significance is not distinguished from statistical significance. When outcome evidence cannot withstand deeper questioning, confidence weakens quickly.
Conclusion
Executing this strategy takes discipline. The discipline to know which assertions you need to invest in and which to deprioritise. The discipline to build evidence across each of the four foundations and to invest in the infrastructure required to do so. It also required the discipline not to make statements you can’t defend. The reward, however, is worth it. Deals will close faster and over time, you’ll become known as a trusted and credible player in the mental health ecosystem. Over time, this will become a strategic asset that creates defensibility. And in this market, that is an important asset.
That’s all for this edition of The Hemingway Report. Many thanks to Jen for sharing these hard-earned insights with us. If you found this Guide valuable, consider supporting our work by becoming a Hemingway Pro Member and joining our community of mental health innovators.
Keep fighting the good fight!
Steve
Founder of Hemingway
